A look at how one dining services team is navigating the realities of the pandemic
“Our focus was on how we could provide safe care not just for our patients, but a safe environment for our staff, for customers and guests,” says Leisa Bryant, director of food & nutrition services.
With advice from MD Anderson’s infection control experts and fellow members of the Association for Healthcare Foodservice (AHF), her team developed a roadmap for how to achieve that goal and navigate the new realities of the pandemic.
For patient dining, the first order of business was a reality check involving production. With the need for social distancing, the kitchen was too small to accommodate a full crew, but fortunately MD Anderson had a spare kitchen that could be drafted into use. Even with that extra capacity, “in terms of space and staff, we realized we could not provide the menu the way it was,” Bryant says. “So the next thing we did was reduce it by 50%.”
Patient choices were curated to include the most popular items, comfort foods like mac and cheese and burgers and selections to accommodate special diets.
To minimize the need for expensive personal protection equipment, patients in isolation have meals delivered by nurses.
With nearly 700 patient beds and 22,000 employees distributed across more than two dozen buildings, the demand for visitor and staff dining is normally robust. In normal times, some 16 cafes, cafeterias, coffee bars and markets satisfy that demand. During the early phases of the pandemic, with visitors extremely restricted, outpatient visits reduced and many staffers ordered to work from home, traffic plummeted.
“We lost 70% or more of revenue,” Bryant recalls. About half of the retail outlets were quickly closed.
Photo: Market baskets—grab-and-go meal kits—have replaced salad bars in one cafeteria. Credit: The University of Texas MD Anderson Cancer Center
The remaining dining facilities were reshaped to reflect government-mandated limits on capacity and social-distancing recommendations. Smaller tables that can seat one or two have replaced larger tables, with 10 to 12 feet between them, and only 20% of the normal seating is available for guest uses. “We allow two people per table if they’re from the same household; otherwise, it’s only one per table,” Bryant says. A supervisor ensures compliance, and a staffer sanitizes tables between guests.
Photo: Tables are restricted to parties of one—two if they are from the same household. Credit: The University of Texas MD Anderson Cancer Center
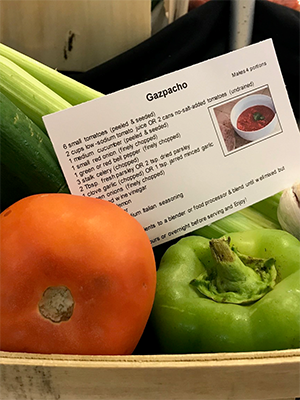
The salad bar and other self-serve stations have been replaced by staff-served dishes or sealed grab-and-go choices. One of the salad bars was converted into a produce market basket—items are packaged with a recipe for preparation at home.
For convenience, a limited supply of staples—milk, bread, rice, cheese, cereal—is available at some retail outlets in the hospital. In addition, the cafes sell to-go packaged prepared meals for a family or single person as a convenience for time-stressed medical and nursing staff. “It helped not only our revenue but kept our team productive,” Bryant says.
An app that employees can use for pickup or delivery orders has been popular and has limited crowding at busy times. The hospital set up a number of delivery points, and orders arrive within 30 minutes. Self-checkouts have also lessened bottlenecks. Grab-and-go items and even hot meals all have a bar code that can be easily scanned and paid for with a credit card.
Photo: Where visitors are allowed, complimentary visitor meals are delivered to patient rooms to minimize unnecessary exposure. Credit: The University of Texas MD Anderson Cancer Center
The shuttered retail facilities have remained closed since April, and the numbers are still down about 65% from normal as many staff continue to telecommute, Bryant says. With work from home expected to continue and be encouraged for the foreseeable future, Bryant says some campus buildings won’t have enough demand to justify a full-fledged dining facility. To serve the needs of staff in those buildings, a ghost kitchen and delivery strategy is under consideration. The hospital had been investigating the idea even before COVID hit.
Meal delivery is likely to play an important role going forward, Bryant says. She also expects contact-free payment and a modest selection of groceries to remain important. Salad bars and other self-serve food stations, on the other hand, are likely gone for good.
Despite the reduction in traffic, the food & nutrition services team has been kept busy, with many of them joining a pool to be cross-trained. Some now transport patients, while others act as a go-between for patients and visitors, who cannot enter many patient areas. “If someone wanted to drop off flowers or a favorite food from home, or a patient wanted a phone charger or other item, we would deliver it,” Bryant says.